Return to Treatments Available
Page
Return to CHC Home Page
New UTube Presentations 12/18: PPC in Cardiovascular Disease PPC - Anti-Oxidant, Anti-Inflammatory, GI, Liver, and Neurologic Benefits
Phosphatidylcholine (PPC/EPL)
Reverse Cholesterol Transport, Cell Membrane Repair, and Atherosclerosis Control
Phosphatidylcholine (specifically 1,2-dilinolenyphosphatidylcholine) is a key component of our anti-atherosclerotic armamentarium (and a component of my personal health-promotion regimen). This molecule, which we will refer to as Essential Phospholipid or PPC, improves cell membrane function, enhancing intake of oxygen and nutrients. PPC stimulates the HDL-associated enzymes of reverse cholesterol transport, promoting the removal of excess cholesterol from our cells, including the endothelial cells that line our arteries. PC has been shown to improve blood flow and reduce symptoms in humans with narrowed arteries, and to anatomically reverse atherosclerotic disease in animals and man.
History and Availability - In Europe, PPC is a pharmaceutical, available under the trade names Lipostabile or N-Essentialle. In researching PPC, I found reference to over 500 papers or abstracts documenting the efficacy of PPC in cardiovascular, neurological, and liver disease. PPC is now off patent, and as such is ignored in standard European medicine (10 years ago I gave a talk in Monaco and most of the doctors in attendance thought that PPC was something new from America). PPC is a distillate of soybean (or sunflower) lecithin, a natural material, and as such PPC cannot be patent protected in the US. No US drug company would or will fund PPC research. Thus, PPC never became a drug in the US, but nutritionally oriented Americans physicians are aware of its anti-atherosclerotic, liver protective, and brain protective benefits. Oral and IV PPC can be legally imported into the US to treat individual patients, and IV PPC is available to US physicians from American compounding pharmacies. This molecule is available in oral form, over-the counter, under the trade names of PhosChol and Plaquex, or admixed with EDTA as LipoPhos EDTA (DeToxMax), a better absorbed and thus more clinically powerful preparation. A low cost approximate of PC can be obtained by taking soybean lecithin and linoleic acid (safflower or sunflower oil) together, the foundation of the Rinse Formula. A booklet describing the Rinse Formula, and Dr. Jacob Rinse, can be found in most health food stores. Dr. Rinse was a brilliant man. He used his knowledge of biochemistry to reverse his own heart disease (at about the time that I was born). Dr. Stephen Sinatra, who I collaborated with in writing Reverse Heart Disease Now, had the privilege of meeting Dr. Rinse.
What is PPC? - Triglycerides, the smallest component of fat, consists of three fatty acids bound to a single molecule of glycerol. Phosphatidylcholine contains two fatty acids and one molecule of phosphocholine (phosphorus attached to choline) bound to the glycerol molecule. The quality of a fat, whether it is good or bad for you, is related to the fatty acids that compose it, be they saturated, unsaturated, or trans. Likewise, the benefit of a phosphatidylcholine is related to its fatty acid components. When both of the fatty acids within a phosphatidylcholine molecule are linoleic acid, that phosphatidylcholine molecule provides unique health benefits, and we refer to this molecule as essential phospholipid or PPC.
How PPC Works -
A. Cell membrane fluidity - The fluidity of the cell membrane, its ability to exchange oxygen and nutrients for carbon dioxide and metabolic waste, to let good things in and convey bad things out, is a function of the fatty materials that comprise it, in turn a function of the type of fatty materials that we take in or manufacture. If our diet is rich in saturated and trans-fats, our cell membranes are stiff and dysfunctional, and we get disease states like diabetes, cancer, and atherosclerosis. The intake of unsaturated fatty acids and phosphatidylcholines, on the other hand, leads to good cell membrane function and vibrant health. Of all dietary and therapeutic fatty materials, none improves cell membrane function as well as does PPC. PPC supplementation improves the status of every cell membrane within our body. As most of our biochemistry is carried out on the cell membrane or on the membranes that cover the organelles (the functional centers within our cells), PPC improves most if not all aspects of our biochemistry. The liver conducts nearly all of its functions on its cell membranes. Thus, it is no surprise that liver disease, any liver disease that you can think of, improves in response to PPC. The choline portion of PPC can be split off and used to make Acetylcholine, a neurotransmitter. As such, PPC is valuable in neurological disease, improving cell membrane function and serving as a precursor for Acetylcholine production.
B. Reverse cholesterol transport - First let's review what we know about cholesterol and cholesterol transport (none of this is covered in drug company TV adds). Cholesterol has been vilified as "the cause" of cardiovascular disease - but that’s not the whole story. Cholesterol is actually a key raw material. Enzymes present in our circulation and in our cells convert cholesterol into Vitamin D, steroid hormones (Estrogen, Progesterone, Testosterone, Cortisol, etc.), and the bile acids that we need for proper digestion. We need some, but not excessive amounts of cholesterol within the semi-permeable membrane that surround our cells. Our body actually runs through about 800 mg of cholesterol each day. If dietary intake of cholesterol drops off, the liver will compensate by making more. Cholesterol itself is not a cause of cardiovascular disease (would Mother Nature provide us with enzyme systems designed to manufacture a raw material that kills us?). Rather, the key problems are excessive cholesterol and/or an inability to process cholesterol properly and/or an inability to guard against oxidation of cholesterol by environmental and endogenous free radicals. Oxidative stress and how we can measure and neutralize it is discussed in other presentations. Here we will talk a little about cholesterol metabolism, how we manufacture it, how we transport cholesterol in our circulation, and how we were designed to transport excessive or “used” cholesterol out of the body.
Cholesterol from the diet travels from the GI tract to the liver, which will also manufacture cholesterol if dietary cholesterol content is limited. Cholesterol, being a fatty material, is not soluble in water, and thus it cannot exist by itself in the blood stream. The liver coats cholesterol with protein, to make a water-soluble LDL-cholesterol lipoprotein, which is then sent out into the circulation. Cells that need cholesterol will display a LDL cholesterol receptor (sort of a molecular open hand) on their cell membrane. The circulating LDL lipoprotein will download a cholesterol molecule to the cholesterol receptor of any cell that needs cholesterol. The cholesterol receptor-cholesterol complex then enters the cell, where the cholesterol is put to good use. Cells that do not need cholesterol will not display the cholesterol receptor on their cell membrane, and thus circulating cholesterol cannot enter cells that don’t need it (think of this feedback mechanism as sort of a cholesterol thermostat). So, no matter how high the blood cholesterol level is, the healthy cell cannot be overfilled with cholesterol (this negative feedback protection breaks down in the presence of oxidative or inflammatory stress – as discussed in other presentations – please review DVD One of the Chronicles of Berberine and the Immune Mechanisms in CV Disease series).
Cholesterol within the vascular wall can bypass the cholesterol receptor and enter vascular cells in excessive amounts if it is oxidized by free radicals. Oxidized cholesterol bypasses the cholesterol receptor and can enter our cells freely, producing cholesterol toxicity. Oxidized cholesterol can and will incorporate itself into the plaque that narrows our blood vessels. Oxidized cholesterol can and will destabilize the plaques, converting a stable plaque into a heart attack or stroke. Cholesterol is not the culprit. Oxidized cholesterol is the culprit. Oxidative and inflammatory stress are the culprits. We know how we can protect against free radical oxidation of cholesterol. First, we can avoid oxidants (i.e. stop smoking). Second, we can remove pro-oxidants from our bodies (i.e. remove Lead and Mercury with EDTA and DMSA). Third, we can take Nrf-2 translocators (such as GlutaClear or Sulfora Clear) which increase the production of our innate antioxidant and detoxification enzymes. Fourth, we can take antioxidants (and here I emphasize a family of antioxidants - the antioxidant defense team), to neutralize free radical oxidants.
While cholesterol itself is not the culprit, cholesterol present in the circulation beyond the body’s needs or within a cell beyond the needs of that cell serves no useful purpose, and it can be oxidized by free radicals. Mother Nature figured this out millions of years ago, so she gave us the ability to carry out Reverse Cholesterol Transport, the ability to remove from our cells (and from the walls of our blood vessels) excessive cholesterol.

To carry out Reverse Cholesterol Transport we need Phosphatidylcholine (PC). PC contains two fatty acids and a phosphocholine group. An enzyme present in our circulation, HDL-associated Lecithin Cholesterol Acyl Transferase (LCAT), removes one fatty acid from Phosphatidylcholine (PC) and attaches it to cholesterol, converting cholesterol into a compound called a cholesterol ester, which is then taken up by a HDL lipoprotein and transported back to the liver, from where the cholesterol is excreted from the body in the form of a bile salt, a digestive enzyme that the liver manufactures from cholesterol (in the presence of Vitamin C). As LCAT converts cholesterol in the circulation into cholesterol ester, it also lowers the content of cholesterol in the blood. A low concentration of cholesterol in the blood promotes the egress of cholesterol out of our cells (including the cells that line our blood vessels), and into the circulation, where LCAT, if enough Phosphatidylcholine is present, will convert this newly mobilized cholesterol into more cholesterol ester, which will be taken up by the HDL and transported out of the body. Reverse cholesterol transport is the means by which Mother Nature removes excessive cholesterol from the body. Reverse cholesterol transport is a means by which Mother Nature keeps our arteries clear of disease. The key enzyme, Lecithin Cholesterol Acyl Transferase, is stimulated by Phosphatidylcholine (particularly if the fatty acids within the PC are linoleic acid, as in the case of PPC), and is poisoned by heavy metals such as Lead, Cadmium, and Mercury.
The reason that your cholesterol level is rising as you age is not because you are lax on your diet (your kids eat junk food and have low BP and cholesterol values - you watch your diet but your BP and cholesterol are rising), but rather due to the progressive loss of enzyme function that occurs due to the progressive heavy metal and overall toxic burden that characterizes the ageing process in our society (LDL production may also increase with age due to oxidative and inflammatory stress – please see the Chronicles of Berberine presentation for a more in depth discussion). LCAT becomes progressively dysfunctional, your HDL particles stop working, you cannot scavenge excess cholesterol from your cells, so you accumulate cholesterol, some of it becomes oxidized (the metals do this as well), and you fill up with plaque and have a heart attack or stroke (and then standard medicine gets involved with drugs and revascularization).
Now, if you supplement with antioxidant vitamins and minerals and remove toxic metals from your body, this process will reverse itself; your enzyme systems come back on line, and you have a chance at restoring your health. In the patient with atherosclerotic vascular disease and pre-existent blockages, we need to take things a step further - we need to stimulate LCAT activity. LCAT activity, this process of reverse cholesterol transport, is stimulated by phosphatidylcholine. If the phosphatidylcholine is PPC, with its two linoleic acids, LCAT stimulation is 100 times greater than in the presence of phosphatidylcholine containing saturated fatty acids. So, if we give you PPC, what will happen? What are the physiological consequences? What happens when we give PPC to individuals with cardiovascular conditions? Take a look below:
|
Enzymes of Reverse Cholesterol Transport or Lipolyis |
PC Effect |
| Lecithin-Cholesterol Acyl-Transferase (LCAT) |
Stimulate |
| Lipoprotein Lipase |
Stimulate |
| Hepatic Triglyceride Lipase |
Stimulate |
|
Lipid Parameters |
|
| Cholesterol, Triglycerides, and LDL Cholesterol | Decreased |
| HDL Cholesterol | Increased |
|
Physiologic Parameters |
|
|
Cell Membrane Function |
Fluidity and Function Improved |
|
Insulin Sensitivity and Diabetes Control |
Improved |
| Blood Viscosity | Decreased |
| Blood Clot Dissolving Capacity | Increased |
| Platelet Aggregation | Decreased |
| Arterial Elasticity | Increased |
| Microvascular and Macrovascular Flow | Increased |
| Redox Capacity | Antioxidant Effect |
| Homocysteine | Decreases |
| Essential Fatty Acid Metabolism | Prostacyclin ↑es and Thromboxane ↓es |
|
Clinical Parameters |
|
| Angina Frequency and Severity | Lessened |
| Treadmill Time and Time to ST Depression | Prolonged |
| Claudication Symptoms | Lessened |
| Lower Extremity and Carotid Blood Flow Measures | Improved |
| Plaque Volume | Lessened |
Can you think of much else to improve? PPC, by improving cell membrane function and by stimulating (HDL and LCAT mediated) reverse cholesterol transport, improves physiologic functions important to the patient with cardiovascular disease, controls risk factors, opens up arteries, improves blood flow, and reverses symptoms.
As stated above, PPC is an extremely effective anti-atherosclerotic therapy. PPC does not interfere with the action of any drug or nutritional (although lipid lowering therapy becomes less important in the patient treated with PPC). PPC does not itself remove heavy metals; rather PPC and chelation therapy are mutually supportive and synergistic. IV PPC is typically administered once or twice a week, over 90 minutes, for 20 to 40 treatments (depending on the extent and severity of your vascular disease), and then monthly to follow. The down side potential of PPC therapy is minimal. PPC has been used IV and orally in Europe for three decades. I've read every paper that I can get my hands on (and abstracts of the papers not written in English), and found a great safety record, and that has been my experience as well. PPC therapy will not be covered by your insurer (again, PPC can't be patented so no research will be done in the US, it will never be a FDA approved drug, so your insurer will not recognize it - but not to worry, they will pay for your open heart surgery and stents, over and over again if required).
 While
I have been impressed with the efficacy of IV and oral PPC, I also realize that
oral uptake of PPC is not efficient. Oral PPC is an oily material, and some
patients have experienced nuisance GI symptoms while taking it.
The
advantage of oral over IV PPC is only one of cost and convenience. A better
compromise is LipoPhos EDTA (or by another manufacturer DeToxMax). In the
preparation of LipoPhos EDTA, the PPC is whipped at high speed, breaking down
the oily material into small particles, small particles that are rapidly
absorbed across the GI tract. These tiny PPC particles also become treatment
delivery vehicles. Any material admixed with the PPC
as it is
being prepared in this fashion can "hitch hike" across the gut wall. EDTA is
only 2-4% absorbed orally, greatly limiting its efficacy when taken by mouth.
EDTA is admixed with PPC during the preparation of LipoPhos EDTA. LipoPhos EDTA
thus provides PPC and EDTA (along with magnesium and lipoic acid) in a readily
absorbable state. Getting back to our biochemistry, our goal here is to
stimulate the activity of HDL-associated LCAT. LCAT is poisoned by heavy metals
and stimulated by PPC. LipoPhos EDTA removes heavy metals and provides PPC.
LipoPhos EDTA preserves and promotes the function of LCAT, reverse cholesterol
transport is enhanced, and arterial health (and your overall health) improves.
While
I have been impressed with the efficacy of IV and oral PPC, I also realize that
oral uptake of PPC is not efficient. Oral PPC is an oily material, and some
patients have experienced nuisance GI symptoms while taking it.
The
advantage of oral over IV PPC is only one of cost and convenience. A better
compromise is LipoPhos EDTA (or by another manufacturer DeToxMax). In the
preparation of LipoPhos EDTA, the PPC is whipped at high speed, breaking down
the oily material into small particles, small particles that are rapidly
absorbed across the GI tract. These tiny PPC particles also become treatment
delivery vehicles. Any material admixed with the PPC
as it is
being prepared in this fashion can "hitch hike" across the gut wall. EDTA is
only 2-4% absorbed orally, greatly limiting its efficacy when taken by mouth.
EDTA is admixed with PPC during the preparation of LipoPhos EDTA. LipoPhos EDTA
thus provides PPC and EDTA (along with magnesium and lipoic acid) in a readily
absorbable state. Getting back to our biochemistry, our goal here is to
stimulate the activity of HDL-associated LCAT. LCAT is poisoned by heavy metals
and stimulated by PPC. LipoPhos EDTA removes heavy metals and provides PPC.
LipoPhos EDTA preserves and promotes the function of LCAT, reverse cholesterol
transport is enhanced, and arterial health (and your overall health) improves.
In practice, in sick individuals who need help in a hurry I will alternate IV PPC and EDTA, 10 to 20 treatments of each, and then switch them to a program of LipoPhos EDTA three days a week and oral PPC the other four days. For prevention, or in stable patients, I will begin with LipoPhos EDTA 2-4 tsp. in juice or water three times a week, for 20-40 weeks, and then 2 tsp. one to two times a week for maintenance therapy. PPC and LipoPhos EDTA is covered in greater detail in our UTube presentation that is available on heartfixer.com. PPC/Lipophos EDTA therapy case studies are also presented within the website Phosphatidylcholine section. Pharmaceutical PPC is a distillate of soy bean oil. Negligible amounts of soy bean protein will be present in PPC, and thus individuals intolerant to soy will likely not have trouble taking PPC.
James C. Roberts MD FACC FAARFM 1/1/20
DeToxMax and EECP in Premature Graft Failure - CA
DeToxMax When and Elderly Patient Refuses Bypass - KC
DeToxMax for Lead Overload and Carotid Disease - KL
DeToxMax as a Chelation Therapy
DeToxMax in Dilated Cardiomyopathy - WJ
Essential Phospholipids in Lipid Control
Essential Phospholipids in Lipid Control in Diabetics
Essential Phospholipids vs. Niacin in Patients with Coronary Insufficiency
Essential Phospholipids and Microcirculatory Blood Flow
Lipostabil in Lovastatin Induced Platelet Dysfunction
Lipostabil in Experimental Diet Induced Atherosclerosis
Lipostabil Regresses Arterial Plaque in Humans
Lipostabil and Lower Extremity Blood Flow
DeToxMax in Progressive Claudication - HD
DeToxMax in Carotid Artery Disease
DeToxMax and EECP in Premature Graft Failure - CA
|
DATE |
EVENT |
| 9/01 | Initial Inferior Wall Heart Attack → Four vessel bypass surgery |
| 12/02 | Adenosine Cardiolite - Global hypokinesis with EF 32%, anteroseptal, inferior, and apical ischemia |
| 1/03 | Angiogram - Three vessel disease: LIMA to LAD graft open, one SVG 60% narrowed and two SVGs closed; PCI not possible |
| 3/03 | Class III symptoms despite maximum medical therapy, requiring 9 NTG tabs/week |
| 1/03 | LAD 50%, Circumflex stent open, with non-dilatable distal RCA narrowings |
| 3-7/03 | 35 hours EECP and 16 weeks of DeToxMax |
| © | Angina resolved; walking three floors without difficulty |
| © | Diabetic neuropathy improved considerably |
| © | Long acting NTG and ACEI stropped as BP fell to low normal |
CA was not experiencing recent good health. This then 71 year old man had sustained a stroke and required surgery to deal with esophageal and prostate malignancies. CA sustained a heart attack in '01; angiography revealed multivessel coronary disease and bypass surgery was carried out. Symptoms recurred in 12/02. An adenosine cardiolite (chemical stress) study revealed pump dysfunction and multiple areas of ischemia, consistent with graft disease. Angiography confirmed the non-invasive findings. Only one graft, the LIMA to LAD conduit, was functioning normally. One vein graft had a 60% narrowing, and two vein grafts had clotted off. Further intervention was not felt to be possible.
CA then came to see me. CA underwent 35 hours of EECP, aiming to improve endothelial function, generate nitric oxide, stimulate collateral flow, and improve pump function. To deal with CA's underlying coronary disease, and his tendency towards disease in general, CA received one bottle of DeToxMax/week over 16 weeks, along with his prior drug regimen and our standard nutritional therapies. This program worked - CA's angina fully resolved; we had to cut back on his meds as CA's BP fell to low normal, and his diabetic neuropathy improved (the lipoic acid in DeToxMax is good for this condition).
12/06 Update - CA has not set foot in the hospital since he began working with me. He took a job out of town and was off his treatment program for about one year, and with this CA's symptoms recurred. We repeated what worked well in '03. CA underwent a repeat program of EECP and he went back on DeToxMax. CA improved again, and will remain on maintenance DeToxMax to help maintain his functional improvement.
When an Elderly Patient Refuses Bypass - KC
|
DATE |
EVENT |
| 9/01 | Initial Inferior Wall Heart Attack → Four vessel bypass surgery |
| 12/02 | Non-Q wave lateral wall heart attack |
| 9/01 | Angiogram - Circumflex 100% with lateral akinesis, 90% LAD, 1st & 2nd diagonal narrowings, RCA 60% and RCA branch 90% lesions. |
|
9/01 ® 3/03 |
IV EDTA x 11 treatments, 4 months of NanobacEDTA, ongoing Beta and Calcium blocker drug therapy, but effort symptoms persistent and calcium score increased from 1522 to 1655. |
| 3/03 | Class III symptoms with an abnormal (modified Bruce) 6:00 stress echo |
| 3-7/03 | 16 weeks of DeToxMax |
| © | Energy level increased |
| © | SBP decreased from 180 to 120 on same meds |
| © | Mowing her lawn with a push mower |
My critics say that I am "anti-medicine" or "anti-bypass". This is a lie. I am personal friends with the best heart surgeon in Toledo and I send him patients all the time. He does his best to help them. I wanted to send him KC but she wouldn't go. Her exact words were "I hear that you've got something better".
KC, then 76, had been troubled by hypertension and a difficult to treat lipid abnormality. Her LDL cholesterol was 240; on top of that her fibrinogen was high at 590 and her homocysteine was elevated at 19. KC sustained a heart attack in 9/01. Angiography demonstrated severe three vessel coronary disease. Bypass surgery was recommended and declined by KC. KC received EDTA chelation therapy, first IV and then as a component of Nanobiotic therapy. Drug therapy was continued along with KC's extensive nutritional regimen. These maneuvers kept KC out of the hospital, but her symptoms did not resolve, and her coronary artery calcium score increased.
I saw KC for the first time in 3/03, and reviewed her 9/01 angiographic findings. A low level stress echo returned abnormal. I recommended repeat angiography and bypass surgery. I felt that KC's heart was just hanging on by a thread, that conservative therapy had not worked, and that bypass surgery was her best option. KC listened to me politely and declined my recommendation. Plan B was to continue her current program and add in DeTox Max. KC was not a good candidate for EECP (I need one good vessel to grow collaterals from) and she lived 90 miles away.
Plan B worked, and it worked beyond my expectations. KC's effort related symptoms improved considerably; her energy level picked up and she was able to mow her front lawn with a push mower. KC has kept up with DeToxMax in a maintenance format, and as far as I know, through 12/06, she continues to do well and has not required a single hospital admission.
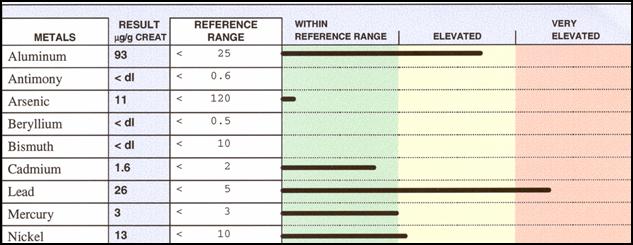
Lead Overload and Carotid Disease - KL
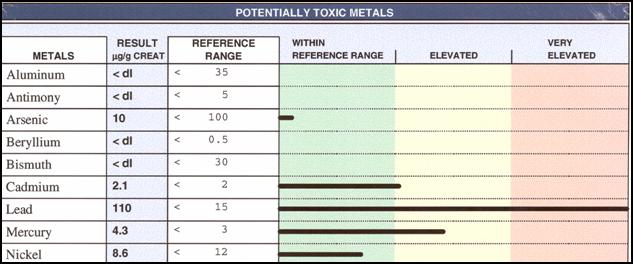
KL presented to me several years ago with dizziness, a low HDL of 30 mg/dl, and a 60% carotid artery narrowing. A Calcium EDTA challenge study demonstrated a lead spill of 110 ug/gram creatinine. KL did not want carotid artery surgery, and we both knew that surgery would not address KL's lead overload, and we both knew that lead was oxidizing KL's LDL particles and poisoning LCAT and the other enzymes of reverse cholesterol transport. KL, then 76 years of age, had owned and managed a gas station, such that he had been repetitively exposed to lead from the gasoline his station pumped. KL received 20 bottles of DeToxMax over 20 weeks and we repeated his challenge study. His post-challenge lead spill had dropped from 110 to 38. His HDL cholesterol rose from 30 to 50. KL received 20 more bottles of DeToxMax, this time spread out over 40 weeks, and his post-EDTA lead spill fell further to 26. His carotid ultrasound picture is stable, a 3:00 stress echo study returned non-ischemic, and KL feels well. KL will keep up with maintenance DeToxMax therapy.
DeToxMax as a Chelation Therapy
Early on I couldn't understand how DeToxMax, which provides only 500 mg of EDTA per dose, could be an effective chelator. EDTA is only 2-4% absorbed when given orally, and while oral EDTA can provide effective lead detoxification, the typical dose here would be 1-2000 mg/day for an extended period of time. How could DeToxMax get anything done, with only 500 mg of EDTA administered orally just twice a week. The key here is the microencapsulated delivery system. We think that these small globules of EDTA, magnesium, and lipoic acid laden PC readily cross the intestinal wall into the blood stream, and then enter the cells of our body. PC is a normal component of the cell membrane, so when the cells take up PC from the PC globules provided by DeToxMax, their "cargo" of EDTA. magnesium, and lipoic acid is dumped into the cells, where the heavy metals are. The worst place within your cell to store heavy metal is the mitochondria, the region where sugar and fat are burned to create ATP energy; unfortunately this is where most of our toxins are stored (so that's why you are so tired). We do know that therapeutically administered PC does get into the mitochondria, so it just may be that EDTA administered within DeToxMax PC also gets into the mitochondria, where we need metal detoxification the most. This theory cannot be proven, but it fits what we are seeing clinically in our patients. A study carried out in another practitioner's office involved the analysis of 24 hour urine specimens from 20 patients, before and after a dose of DeToxMax. The chart below gives you the results. Metals came out, and they came out over several days. In my mind I see the EDTA molecules contained in DeToxMax roving the body, searching for and then binding toxic metals, then ferrying them out of the body via the urine and GI tract.
DeToxMax in Dilated Cardiomyopathy - WJ
I feel that dilated cardiomyopathy, heart failure due to generalized weakness of the heart muscle, is due predominately to heavy metal overload. We are seeing more and more cardiomyopathy, in younger and younger patients, and unfortunately this trend will continue (until our society and our medical profession decide to recognize the problem). If you do heart muscle biopsy studies of cardiomyopathy patients, you will find tissue mercury levels 22,000 times above that found in normal individuals. The cardiomyopathy patients also have greatly increased heart muscle tissue levels of antimony, arsenic, and other metals. I think that patients with dilated cardiomyopathy have a genetic or acquired inability to defend themselves against environmental metal toxins (similar to the situation with mercury in autistic kids). Much of the benefit of MME in cardiomyopathy has to do with metal detoxification. I have also used other forms of chelation therapy to improve pump function in cardiomyopathy patients (most but not all improve - in some the problem is likely something other than a metal that we can chelate out). Here we describe improvement in pump function in a patient treated with DeToxMax.
|
DATE |
Event | LVd | EF | EPSS |
| 8/01 | Atrial flutter at 150 with CHF | 7.3 | 25% | 2.5 |
| 4/02 | Sinus rhythm on amiodarone and ACEI | 7.1 | 40% | 1.8 |
| 9/03 | 10 bottles of DeToxMax | 6.2 | 55% | 0.6 |
| 2/04 | 20 bottles | 5.4 | 55% | 0.9 |
WJ, a then 78 year old non-hypertensive, non-diabetic, amalgam bearing former smoker presented to me in 8/01 with atrial flutter and a heart rate of 150. His heart was overworking at this abnormal heart rate, burning off its ATP energy pool. WJ's heart was dilated (normal is a diastolic dimension of £ 5.6 cm), his EPSS was increased at 2.5 (a reproducibly echo measure of pump function - normal is £ 1.0), and his ejection fraction was only 25% (normal is ³ 50%). Electrical cardioversion combined with amiodarone, our most effective anti-arrhythmic agent, returned WJ's heart rhythm back to normal, and I added a tissue specific angiotensin converting enzyme inhibitor (a standard therapy for cardiomyopathy, discussed in the Drug Therapy for CHF section of this website), but WJ's heart remained enlarged and dysfunctional. WJ would not allow me to carry out a diagnostic triple challenge study, but based on our knowledge of the relationship between metal overload and cardiomyopathy, some form of metal detoxification made sense to me. WJ received DeToxMax and his cardiomyopathy picture resolved. WJ remains on maintenance DeToxMax, one bottle a month, and through 12/06 he has not required a cardiac admission; pump function remains improved and atrial flutter has not recurred. When you remove the cause of disease, the disease tends not to recur. When you remove the cause of disease, you don't have to resort to repetitive invasive procedures to deal with the consequences of the cause of a disease state (I know, I know, this is all politically incorrect and not the standard of care and it upsets your other physicians, but sometimes I just can't help myself - I forget that I am a Fellow of the American College of Cardiology, and instead of using only drugs and surgery as I was taught, I use my mind and the science available to actually address the underlying cause of your illness). DeToxMax helps me here.
Essential Phospholipids in Lipid Control
This study was carried out with the European (Lipostabil) drug form of PC. Patients with hyperlipidemia were randomized to receive 1800 mg/day of oral PC or placebo over a six week period, within a double blind protocol (neither the subjects nor the investigators knew who was receiving PC or placebo). The results are presented in graphic form on PC in Lipid Control Graphic. Basically, lipid values were unchanged with placebo therapy while with PC, Cholesterol fell 20%, from 309 to 250, LDL by 32%, from 192 to 131, triglycerides by 30%, form 354 to 249, while HDL rose by 30%, from 36 to 53.
Essential Phospholipids in Lipid Control in Diabetics
Thirty adults with medically controlled type II diabetes were randomized to receive over four weeks 900 mg of Lipostabil PC three times a day, or placebo, again in double blind format. Fasting blood sugar fell slightly in both groups; HbA1c was unchanged with placebo therapy but fell from 7.9 to 7.3 with real PC. Lipid changes are presented graphically on PC in Diabetic Lipid Control. Lipostabil worked in diabetics just as well as it did in the non-diabetics. Of interest, while the lipid lowering drugs that we force on you often cause nuisance (and sometimes more than nuisance) side-effects, two thirds of the diabetics assigned to Lipostabil reported a significant overall improvement in their sense of well being.
Essential Phospholipids vs. Niacin in Patients with Coronary Insufficiency
100 subjects with hyperlipidemia, coronary disease with effort angina and and abnormal bicycles stress EKG, were placed on a low cholesterol, low fat diet. Lipid lowering drugs were stopped. Four weeks later the subjects were randomized to receive over six months either niacin at a dose of 500 mg three times a day or Lipostabil, 500 mg/day IV over 14 days followed by 1,800 mg/day orally for 5 & 1/2 months. The results are presented graphically on PC vs. Niacin Graphics.
Niacin has a slight edge over Lipostabil (here abbreviated as EPL, short for Essential Phospholipid) with respect to lipid control, but EPL was better tolerated. Both had an anti-oxidant effect, lowering levels of conjugated diene and hydroxyperoxides in the circulation (markers of free radical damage), but EPL had the edge with respect to hydroxyperoxide reduction. This isn't just esoteric biochemistry - remember it is only the oxidized LDL that can hurt you. EPL lowers not just the LDL value, but it lowers the level of free radical stress, a double benefit. Stress test parameters improved with both Niacin and EPL therapy, with EPL having an edge, and EPL was of greater benefit in reducing anginal symptoms.
Niacin improves outcome in patients with coronary disease, and from the above study you can see why. This study compared the results of two good therapies (many of my patients take both). EPL is not quite as effective as is niacin in lipid control, but it is definitely better tolerated. Both therapies blunt oxidative stress, improve stress test findings, and reduce ischemic symptoms, with EPL the more effective of the two.
Essential Phospholipids and Microcirculatory Blood Flow
This is a really cool study; it illustrates what PC is doing at the microcirculatory level. Thirty patients with coronary or carotid artery disease received Lipostabil, 250 mg/day IV over 30 days. Photomicrographs of their conjunctival (inner lining of the eyelid) were obtained at baseline and at 30 days. The findings are presented below in table form:
| Baseline | 30 Days | % Change | |
| Arterial Diameter | 1.4 | 3.1 | 124% |
| Vein Diameter | 2.1 | 3.5 | 66% |
| Capillary Diameter | 1.5 | 3.4 | 127% |
| Collaterals | 1.3 | 3.5 | 165% |
| RBC Aggregation | 2.9 | .6 | -79% |
| Baseline | 30 Days | % Change | |
| Platelet Aggregation | 3.4 | 1.4 | -59% |
| Clot Formation Time | 3.2 | 4.6 | 44% |
| Euglobulin Lysis | 38 | 44 | 16% |
| RBC Deformability | 11.8 | 13.8 | 17% |
| Blood Viscosity | 12.3 | 10.7 | -13% |
In response to PC therapy, blood vessels dilate and collateral vessels enlarge (thus PC should improve one's response to EECP and that has been my experience). Cell membrane function improves, so red cells are more deformable, more likely to wiggle through capillaries and transport their oxygen to the cells that need it, and less likely to aggregate and sludge. Platelet membrane function is improved (platelets rich in oxidized cholesterol are more likely to clot while those with a lot of PC in their membrane are less likely to aggregate into a clot). Blood is less viscous (more like wine and less like catsup) and flows easier. Clots form less readily, and any clot that does form dissolves more rapidly. Isn't this a great molecule!
Lipostabil in Lovastatin Induced Platelet Dysfunction
This study will not be shared with your other doctors during lunch provided by a drug rep. Lipid and platelet function studies were obtained in 18 hyperlipidemic coronary patients before and after a 4 week program of Lovastatin (the generic name for Mevacor; the starting dose was 20 mg/day, increasing as tolerated to achieve and on-treatment cholesterol of £ 200 mg/dl).
Cholesterol fell, as expected, from 319 to 209, and LDL from 227 to 132, but platelet function worsened. The graph below describes the percentage of platelets that spontaneously clump into aggregates when placed in suspension; this parameter worsened by 76%. ADP, released by oxygen starved cells that cannot regenerate their ATP energy supply, promotes platelet aggregation and clotting, and does so more readily in the Lovastatin treated patient.
If we lower cholesterol with other therapies, especially PC, platelet aggregation and clot forming tendency decreases, but with Lovastatin the opposite is occurring. OK, what can we do about this? There are benefits associated with statin therapy (and other statins may not have this deleterious effect on platelet function). Can we neutralize this side-effect of Mevacor?
In an in vitro (test tube) study, platelet aggregation rate was studied in whole blood, with and without Lovastatin and several other treatments.
Whole blood incubated with a clinically relevant level of Lovastatin demonstrates an increased tendency towards platelet clot formation, a bad thing. Whole blood mixed with the plasma of an individual not receiving Mevacor does not clot abnormally, while plasma drawn from a Lovastatin-treated patient increases the platelet clotting rate. Thus there is something missing from the plasma of a Lovastatin-treated patient or something abnormal in the plasma of a Lovastatin-treated patient that is disturbing platelet membrane physiology and promoting platelet clot formation. We know that PC (EPL in the graph) improves platelet function and decreases the tendency of platelets to aggregate. The fifth column shows what happens with whole blood is incubated with clinically relevant concentrations of Lovastatin and EPL. EPL not only neutralizes the platelet clot forming effect of Lovastatin, it decreased the platelet aggregation rate to below baseline - what a powerful therapeutic effect.
Lipostabil in Experimental Diet Induced Atherosclerosis
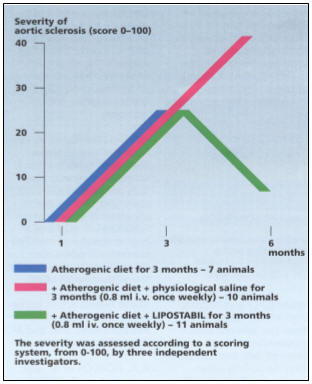
In this study Quail were fed an atherogenic diet rich in oxidized saturated and trans-fats. 1/3rd were sacrificed and the severity of aortic plaque graded on a 0-100 scale. The remaining birds were maintained on the same plaque producing diet, along with Lipostabil, 200 mg IV once a week, or IV saline administered once a week as a control substance. At six months the birds were sacrificed and their aortas' examined for plaque buildup.
Lipostabil exerted a dramatic anti-atherosclerotic effect. In red are the birds assigned to three months of the plaque producing diet; their aortas began to fill up with plaque. Six months of the same diet (red line) led to more extensive disease. But six month of the bad diet, with Lipostabil over the final three months, was associated with only minimal disease. Lipostabil regressed the disease that had built up with three months of the atherogenic diet, even as this plaque producing diet was continued. This really shouldn't come as a surprise to you. Remember, PC stimulates reverse cholesterol transport and has an antioxidant effect. We don't want you to follow a bad diet, but none of us are perfect and PC seems to work (at least in this study), even in the presence of a disease producing diet.
Lipostabil Regresses Arterial Plaque in Humans
 This study was not published in English; its abstract was and I obtained the
graphic from the Lipostabil monograph published by Rhone-Poulenac Roher, the
European manufacturer of Lipostabil. This monograph contains 197 references
from the European and Russian medical literature. In this study, completed
in 1989, 15 humans with early, asymptomatic atherosclerosis received 2,700
mg/day of oral Lipostabil over twelve months. Plaque volume within their carotid and femoral
arteries was measured by ultrasound every three months:
This study was not published in English; its abstract was and I obtained the
graphic from the Lipostabil monograph published by Rhone-Poulenac Roher, the
European manufacturer of Lipostabil. This monograph contains 197 references
from the European and Russian medical literature. In this study, completed
in 1989, 15 humans with early, asymptomatic atherosclerosis received 2,700
mg/day of oral Lipostabil over twelve months. Plaque volume within their carotid and femoral
arteries was measured by ultrasound every three months:
Plaques > 25 microliters in size are depicted in red and those < 25 microliters in size are in blue. With oral Lipostabil, the initially smaller plaques increase only minimally in size and then stagnate. The larger plaques initially increase in size (which may be their natural history), and then regress.
In other words, Lipostabil regresses arterial plaque in humans!
If this phenomena was demonstrated in 1989, why aren't we using Lipostabil in medicine today? The reason, I believe, has to do with money. Lipostabil is no longer on patent, it is available in generic form here and in Europe, so no entity stands to profit from research dollars spent on PC research. The European drug companies can make money off their new drugs, and that is what they are going to do. Capitalism is a wonderful thing, but here it doesn't lend itself well to optimizing world health. There was a great buzz several years ago regarding a new drug that regressed plaque in humans by 2% following IV administration. The small company studying this new drug was promptly taken over by one of the pharmaceutical giants. When the paper came out I actually read it. Buried in the methods section was a description of the vehicle in which the new drug was administered. Guess what it was - it was unsaturated phosphatidylcholine - in other words PC. As the drug industry has now found a way to bring PC back in a patentable, profitable form, it just might make its way into standard American medicine. Good thing we have it now as good old PC.
Lipostabil and Lower Extremity Blood Flow
Lower extremity blood flow, at rest and following effort, was measured in normal volunteers and in individuals with mild to moderate or advanced lower extremity vascular insufficiency, at baseline and following 30 days of oral Lipostabil 900 mg taken three times a day.
|
Volume of lower extremity blood flow (ml/100 gm muscle/min.) |
||||||
| Resting blood flow | Post-exercise blood flow | |||||
| Baseline | 30 days | % change | Baseline | 30 days | % change | |
| Normal Volunteers | 2.3 | 2.6 | 13% | 32 | 33.5 | 3.4% |
| Mild-mod. Disease | 1.5 | 1.75 | 17% | 21.7 | 24.2 | 12% |
| Advanced Disease | .9 | 1,1 | 23% | 13.8 | 15.7 | 21% |
As you can see, the normal volunteers became a little more normal, while lower extremity blood flow improved in the subjects with pre-existent disease with only 30 days of oral Lipostabil. How will this correlate with effort capacity and claudication symptoms?
Pain free treadmill walking time was assessed in 808 patients at baseline and after 6 weeks of oral Lipostabil, 1,800 mg/day .
Mean pain free walking time increased from 9.8 to 21.3 minutes. Amongst the 808 patients, 505 with pre-treatment rest pain reported complete relief of this symptom. 198 with intermittent claudication reported complete relief. Only 105 or the 808 study patients remained symptomatic. I wonder how DeToxMax will do in patients with peripheral vascular disease?
DeToxMax in Progressive Claudication - HD
This then 74 year old woman with multiple risk factors (cholesterol 368, Lp(a) 38, homocysteine 14, triglycerides of 612, and prior amalgam fillings) was facing surgery to address progressive claudication. This is no longer the case, thanks to DeToxMax.
|
DATE |
EVENT |
| 6/95 | Asymptomatic PVDz: Right ABR .76 and Left .71 |
| 11/98 | Symptomatic (LDL 98 on statin): Right ABR .44 and Left .41 |
| 5/03 | Pentoxifylline not effective Right .30 ® .27 with exercise and Left .27 ® .21 |
| 6/03 | Arginine poorly tolerated; statin stopped due to cost - distal pulses now absent |
| 8/03 | Six bottles DeToxMax and claudication improved |
| 6/04 | 30 bottles ® Claudication resolved and cholesterol down to 190 mg/dl, and ABR: |
HD was worsening, despite politically correct statin therapy that she really couldn't afford. Pentoxifylline wasn't effective and HD could not tolerate arginine. With just 6 bottles of DeToxMax, taken over 6 weeks, HD noted a reduction in effort related leg pain. After thirty bottles claudication became a non-issue; the same for her lipid abnormality. Lower extremity blood flow, which had been steadily worsening, improved with DeToxMax (the ankle-brachial ratio is discussed on the Diagnostic Studies Available page of this website).
DeToxMax in Carotid Artery Disease
SR is not my personal patient, but I did review his clinical history and carotid ultrasound reports, which show a striking response to DeToxMax therapy. This 77 year old man with poorly controlled diabetes and liver disease presented in 5/03 with sudden loss of vision in his right eye. Ultrasound study revealed severe carotid artery disease, with subtotal occlusion of the right carotid. SR declined surgery, and instead was treated with 24 bottles of DeToxMax, plus Nattokinase (digests fibrinogen and fibrin blood clots) over 12 months. Vision was not restored (SR had sustained a stroke with irreversible damage), but his one year carotid ultrasound showed marked improvement.
|
DATE |
EVENT |
| 5/03 | Visual loss in right eye |
| 5/03 | Severe disease RICA and LICA - no flow beyond mid-point in RICA |
| 5-11/03 | 24 bottles of DeToxMax plus Nattokinase therapy |
| 11/03 | Vision no better |
| 11/03 | LICA - 50-69% narrowing RICA - No pressure step up; only non-obstructive disease identified |
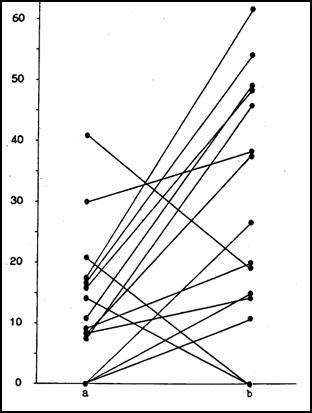
With this fantastic outcome in mind, an informal study was carried out with six of my personal patients. Carotid ultrasound exams were carried out before and after a 20 week treatment program consisting of DeToxMax, 1/2 bottle twice a week, and Lumbrokinase, 2 capsules three times a day over the first month and one capsule three times a day over the following 16 weeks. These were not the healthiest subjects, and all had previously been treated for atherosclerotic vascular disease. Two had received prior IV EDTA chelation, five had received EDTA as a component of NanobacEDTA treatment, and five had required EECP for refractory angina. All had undergone a prior ultrasound. The carotid ultrasound is discussed on the Diagnostic Studies Available page. With this methodology, the greater the flow velocity, the tighter is the carotid narrowing. A drop in velocity indicates that blood flow has improved, that the artery is opening up. Our findings are presented on DeToxMax Carotid Graphics.
20 weeks of DeToxMax plus Nattokinase improved blood flow in the carotid arteries of my patients. Patients whose arteries are opening up do not have events; they do not require hospitalization and they do not need invasive procedures. PC and EDTA are great therapies, and DeToxMax combines them in an easy to take, oral format. I love this stuff.
James C. Roberts MD FACC
12/07/06